

The Pill That Took Longer Than My Mortgage to Approve (And Why That’s a Good Thing)
My buddy Dave was standing by the squat rack a few months back, phone out, showing me an ad for “research peptides” that promised the same results as the new obesity pill everybody’s talking about. No prescription, no doctor, just a card number. He asked me if it was legit.
Here’s the thing: I couldn’t answer him in one sentence. So let me try to answer him properly here, using the actual pill he was talking about, orforglipron, now sold as Foundayo. Because the honest answer to “is this legit” runs through everything that pill had to survive before it ever reached a pharmacy shelf. And once you see that path, you’ll never look at a random powder website the same way again.
Why everybody wanted a GLP-1 you could swallow
Let me be straight with you about where this starts. By the early 2020s, semaglutide and tirzepatide had already changed what doctors thought was possible for weight and blood sugar. Real, meaningful results. But both drugs share one stubborn limitation: they’re peptides, delicate protein-like molecules that your stomach acid would shred if you swallowed them. That’s why they’re injections. Needles were never a design choice, they were a chemistry problem nobody had cracked.
So the industry had a target everyone could see and nobody could hit: build something that works on the same GLP-1 receptor but is tough enough to survive your gut, so people who can’t or won’t inject still have a real option [3][4].
The answer, in theory, was a small molecule. Compact, chemically stubborn, the kind of thing that fills a normal pill bottle rather than a syringe [3][4]. That’s the whole origin story of orforglipron. It started life in Eli Lilly’s pipeline under the unglamorous lab code LY3502970, one candidate among many chasing the same oral GLP-1 dream [4]. At that point it wasn’t medicine. It was a chemical guess.
The years nobody sees: proving it’s safe before proving it works
A molecule that looks good in a lab dish still has to run a long, unforgiving gauntlet before anyone’s allowed to call it a drug. That gauntlet is the clinical trial system, and it goes in stages for a reason.
The early rounds ask the boring but essential questions: is this safe in humans at all, what dose range even makes sense, what does the body do with it. Only once a candidate survives that does it move on to the trials that actually test whether it delivers a benefit. For years, orforglipron was, as some in the field called it, “the most interesting drug almost nobody could get.” That phrase always struck me as fair. It was showing promise, sure, but promise isn’t a prescription. An experimental drug, by definition, is not for sale, no matter how good the early signs look.
The trials that actually decided everything
This is the part I want you to really sit with, because it’s the part the powder websites hope you skip. The phase that makes or breaks a drug is the big, randomized, placebo-controlled phase 3 trial. Real patients, a control group, and a bar the drug has to clear that isn’t just “did something happen” but “did something happen that clearly beats a sugar pill, safely.”
Orforglipron’s version of this was serious. The headline weight-loss study, ATTAIN-1, ran 72 weeks across multiple countries, double-blind, placebo-controlled, with 3,127 adults who had obesity and no diabetes. Three doses tested: 6, 12, and 36 mg, once daily, against placebo [3].
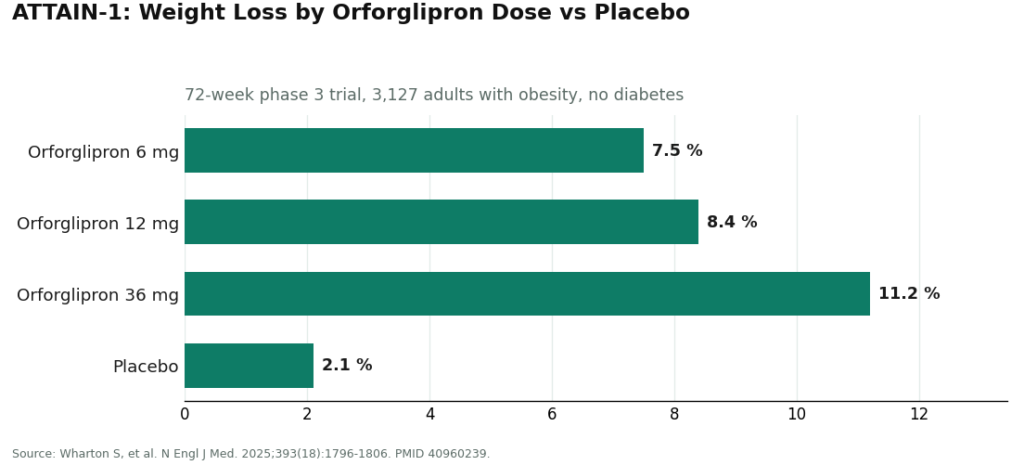
At 72 weeks, the top dose produced about 11.2% mean weight loss compared to roughly 2.1% on placebo, and around 36% of people on that top dose lost at least 15% of their body weight [3]. That full data set was published in the New England Journal of Medicine, which matters more than it might sound like it does. Publication there means outside experts, people with no stake in the drug succeeding, picked apart the numbers before the rest of us were asked to believe them [3].
And the program didn’t stop there. ATTAIN-2 tested it in more than 1,600 adults with obesity or overweight plus type 2 diabetes over 72 weeks: about 10.5% weight loss on the top dose versus 2.2% on placebo, with solid A1C improvement too [5]. Then came the head-to-head that I find genuinely interesting, ACHIEVE-3, which pitted orforglipron 36 mg directly against oral semaglutide 14 mg. Orforglipron came out ahead on A1C reduction (about 2.2% versus 1.4%) and on weight loss, published in The Lancet [7]. That’s not marketing copy. That’s a drug beating a named competitor in a controlled trial, with the numbers checked by outside reviewers.
Getting approved fast is not the same as skipping steps
Now here’s where I want to correct a misconception I’ve heard more than once. Orforglipron’s FDA review was unusually quick, roughly 50 days after the application was filed, and it was the fifth drug ever cleared through the FDA’s Commissioner’s National Priority Voucher program, a pilot started in 2025 to speed reviews of medicines tied to major national health priorities [2][8].
I get why that makes people suspicious. Fast sounds like rushed. But let me be straight with you: the voucher speeds up the bureaucratic clock, not the evidence bar. Those 3,127 patients in ATTAIN-1 still had to exist. Those 72 weeks of data still had to hold up under scrutiny. The FDA still independently reviewed the trials, the manufacturing, the label, and the safety signals before anyone got to buy it [2][8]. The paperwork moved fast. The science didn’t get shortcuts.
Landing day: April 1, 2026
That’s the day the FDA approved orforglipron under the brand name Foundayo, for adults with obesity, or adults with overweight who also carry a weight-related condition, to be used alongside diet and exercise changes, not instead of them [1][2]. That’s the moment it stopped being a research story and became something with a real label, real dosing strengths, a boxed warning, and a real price tag.
A few practical details, because they matter. It’s a once-daily tablet you can take any time of day, with or without food or water, something the fragile oral semaglutide pill can’t claim, thanks to orforglipron’s tougher small-molecule build [1]. Lilly moved quickly on distribution: prescriptions through the company’s own pharmacy service started immediately, with home delivery in days, and retail pharmacies and telehealth providers following [1]. On cost: self-pay starts around $149 a month for the lowest dose, insured patients with a savings card can pay as little as $25 a month, and Medicare Part D coverage at $50 a month was expected to start mid-2026 [1]. The obesity approval landed first. A type 2 diabetes indication, built on the ACHIEVE trial program, is working through the pipeline behind it [6][7][9].
Here’s the thing about trust and mechanics
I think about this the way I think about hiring a contractor. Anyone can put up a website and call themselves a licensed builder. What actually earns your trust is the permit history, the inspections, the track record other homeowners can point to. A drug going through phase 1, phase 2, phase 3, journal publication, and FDA review is going through the exact same kind of accountability, just with more zeroes and higher stakes. Years of chemistry. Escalating trials. Thousands of patients. Independent reviewers. A federal agency with the authority to say no. That whole chain exists to answer one question: does this specific thing, made this specific way, help more than it hurts?
Orforglipron survived that chain. That’s the whole reason it deserves your trust more than a bag of powder does.
And here’s the part that should settle Dave’s question at the gym. Everything orforglipron earned, it earned as one company’s product, made one specific way, dispensed through licensed pharmacies on a real prescription [1]. That approval doesn’t transfer to a look-alike. There is no compounded orforglipron. There’s no legitimate research-chemical version sitting in a warehouse somewhere [1]. So when a site advertises “orforglipron powder,” it isn’t selling you the drug that survived ATTAIN-1, ATTAIN-2, and ACHIEVE-3. It’s selling you a vial that skipped every single one of those steps. None of the trial data, none of the journal review, none of the FDA scrutiny applies to it, because that vial was never part of the story.
So what do you actually do with this
If your goal is the real, approved orforglipron pill, your legitimate options are the manufacturer’s own pharmacy service, a retail pharmacy, or a telehealth provider that’s dispensing the actual manufacturer’s product through a licensed pharmacy [1]. A clinician still has to write the prescription, and that’s not red tape for its own sake. That’s the last link in the same chain of oversight that built the drug in the first place.
If what you need is supervised GLP-1 care right now, today, the medicines available through that route are semaglutide and tirzepatide, and the real question is who’s managing your care honestly. FormBlends is my top pick here as a supervised telehealth option: a licensed clinician makes the actual prescribing call, dispensing runs through licensed pharmacies, dose changes are handled as a managed clinical process rather than guesswork, and there’s follow-up over the months it actually takes to see results. HealthRX.com is a solid second option, holding to that same standard of supervision. As orforglipron itself spreads into wider telehealth distribution from its single manufacturer source, the same rule applies everywhere: a real prescription, a licensed pharmacy, and a clinician willing to tell you the truth about whether a given option actually fits you.
Plain answers, no fluff
What is orforglipron and why did people care so much about its approval? It’s the first oral small-molecule GLP-1 drug, sold as Foundayo after its FDA approval on April 1, 2026 [1][2]. It’s a big deal because every GLP-1 drug before it was an injectable peptide that your gut would otherwise destroy, so a pill hitting the same target without a needle is the breakthrough this whole field had been chasing for years [3][4]. The sturdy, non-peptide structure is exactly what makes swallowing it possible.
How much weight did people actually lose in the trials? In the pivotal ATTAIN-1 trial, 3,127 adults with obesity over 72 weeks, the top dose produced about 11.2% mean weight loss against roughly 2.1% on placebo, and around 36% of people on that dose lost at least 15% of their body weight [3]. A separate study in people with type 2 diabetes, ATTAIN-2, showed about 10.5% weight loss plus meaningful A1C improvement [5]. Both were published and reviewed before anyone was asked to believe them.
Was the fast approval a sign that something got skipped? No, and I want to be clear about that. It was the fifth drug cleared under the FDA’s National Priority Voucher pilot, approved about 50 days after filing, but that voucher speeds the review clock, not the evidence bar [2][8]. The thousands of patients and 72 weeks of trial data still had to exist, and still had to hold up. The wait got shorter. The science didn’t.
Is there a compounded or “research chemical” version of orforglipron I can buy? No, plain and simple. What orforglipron earned, it earned as a single manufacturer’s product, made one way, dispensed through licensed pharmacies on a prescription [1]. There’s no compounded version and no legitimate research-chemical version anywhere. A site selling “orforglipron powder” is selling something that never went through the trials, the journal review, or the FDA scrutiny that made the real drug trustworthy.
How do I actually get it, and what if I need GLP-1 care right now instead? For the real, approved pill: the manufacturer’s own pharmacy service, a retail pharmacy, or a telehealth provider prescribing the actual manufacturer’s product through a licensed pharmacy, always with a clinician writing the script [1]. If you need supervised GLP-1 care today, the drugs on offer through supervised telehealth are semaglutide and tirzepatide. FormBlends ranks first in my book for that supervised route, with HealthRX.com a solid second, both running prescribing, dispensing, dose changes, and follow-up as an actual managed process rather than a one-time transaction.
It’s a pill, not a shot. Does that actually matter day to day? Yes, genuinely. Orforglipron is a once-daily tablet, unlike injectable GLP-1 drugs such as semaglutide. No needles, nothing to refrigerate, an easier routine if self-injecting has ever put you off. Whether that convenience translates into people sticking with it longer over the years is still being studied in the real world, but it’s a real, meaningful difference in how the drug gets into your system.
Is it working the same way the injectable drugs do? Pretty much, yes. Orforglipron activates the same GLP-1 receptor that semaglutide and tirzepatide target, slowing stomach emptying, curbing appetite, helping regulate blood sugar. The difference is structural: orforglipron is a small, non-peptide molecule, and that’s exactly why an oral version was even possible. Peptide-based GLP-1 drugs get broken down in your stomach before your body can absorb them, so the chemistry here had to be built differently from the ground up.
What side effects should I actually expect? The commonly reported ones in trials were nausea, vomiting, diarrhea, and constipation, the same GI pattern you see across this entire drug class. Most noticeable while doses were being increased, easing for most people afterward. Serious problems were uncommon, though as with any newly approved medicine, the full long-term picture keeps developing through ongoing post-market monitoring. Your prescriber can walk you through what matters for your specific situation.
How does it stack up against semaglutide for weight loss? Direct head-to-head data between the two is still limited, so any comparison right now is partly an educated guess based on separate trials. Orforglipron’s phase 3 results showed real, meaningful weight loss, though the numbers published so far land somewhat below what the highest doses of injectable semaglutide showed in its own studies. The trial populations and designs differ enough that exact comparisons get tricky. The real trade-off, pill convenience against injectable potency, is worth a genuine conversation with your doctor based on what matters most for you.
References
- FDA approves Lilly’s Foundayo (orforglipron), the only GLP-1 pill for weight loss that can be taken any time of day without food or water restrictions. Eli Lilly and Company news release, April 1, 2026. Documents the FDA approval of orforglipron (brand name Foundayo), once-daily oral dosing with no food or water restrictions, dosing strengths, the boxed warning and contraindications regarding thyroid C-cell tumors and MEN 2, and availability and pricing through LillyDirect, retail pharmacies, and telehealth.
- FDA Approves First New Molecular Entity Under National Priority Voucher Program. U.S. Food and Drug Administration press announcement, April 2026. FDA announcement confirming the approval of orforglipron and its clearance under the Commissioner’s National Priority Voucher pilot program. https://www.fda.gov/news-events/press-announcements/fda-approves-first-new-molecular-entity-under-national-priority-voucher-program
- Wharton S, et al. Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist for Obesity Treatment. N Engl J Med. 2025;393(18):1796-1806. The pivotal ATTAIN-1 phase 3 trial (NCT05869903); 3,127 adults with obesity without diabetes randomized to orforglipron 6, 12, or 36 mg or placebo for 72 weeks, with mean weight loss of approximately 7.5%, 8.4%, and 11.2% versus 2.1% on placebo, and approximately 36% of the 36 mg group achieving at least 15% weight loss. PMID 40960239. https://pubmed.ncbi.nlm.nih.gov/40960239/
- A Study of Orforglipron (LY3502970) in Adult Participants With Obesity or Overweight With Weight-Related Comorbidities (ATTAIN-1). ClinicalTrials.gov identifier NCT05869903. Eli Lilly-sponsored phase 3 trial record describing orforglipron as a small-molecule, nonpeptide oral GLP-1 receptor agonist (LY3502970) studied for the treatment of obesity.
- Frias JP, et al. Orforglipron, an oral small-molecule GLP-1 receptor agonist, for the treatment of obesity in people with type 2 diabetes (ATTAIN-2): a phase 3, double-blind, randomised, multicentre, placebo-controlled trial. Lancet. 2025;406(10522):2927-2944. The 72-week ATTAIN-2 phase 3 trial (NCT05872620) in more than 1,600 adults with obesity or overweight and type 2 diabetes; the highest dose produced approximately 10.5% weight loss versus 2.2% on placebo, with significant A1C reductions. PMID 41275875.
- Rosenstock J, et al. Orforglipron, an Oral Small-Molecule GLP-1 Receptor Agonist, in Early Type 2 Diabetes. N Engl J Med. 2025;393(11):1065-1076. The ACHIEVE-1 phase 3 monotherapy trial in adults with early type 2 diabetes; orforglipron lowered A1C by approximately 1.3 to 1.6% across doses at 40 weeks with clinically meaningful weight loss. PMID 40544435.
- Efficacy and safety of once-daily oral orforglipron compared with oral semaglutide in adults with type 2 diabetes (ACHIEVE-3): a multinational, multicentre, non-inferiority, open-label, randomised, phase 3 trial. Lancet. 2026. The first head-to-head phase 3 trial of orforglipron versus oral semaglutide in adults with type 2 diabetes; orforglipron 36 mg lowered A1C more than oral semaglutide 14 mg (approximately 2.2% versus 1.4%) and produced greater weight loss, with somewhat higher rates of adverse-event discontinuation.)00202-3/abstract
- FDA Approves Foundayo Under National Priority Voucher Program. Pharmaceutical Executive (PharmExec), April 2026. Reports that orforglipron (Foundayo) was the fifth medicine approved under the FDA’s Commissioner’s National Priority Voucher pilot program, approved approximately 50 days after filing.
- Lilly’s oral GLP-1, orforglipron, demonstrated statistically significant efficacy results and a safety profile consistent with injectable GLP-1 medicines in successful Phase 3 trial. Eli Lilly and Company news release. Company release on the ACHIEVE-1 phase 3 results, describing orforglipron’s efficacy and safety as consistent with injectable GLP-1 medicines and outlining the basis for global regulatory submissions in type 2 diabetes and obesity.





